Now we are post-eclipse. If you or anyone you know is noticing a new difficulty reading with their central vision today (Wednesday, two days after the eclipse), and they spent some time watching the solar eclipse without solar safety glasses, then it's time to visit an optometrist or ophthalmologist for a retinal exam.
You can learn about how and why the light from the Sun can burn or damage the very important photoreceptor cells in your retina here where I was interviewed by Rachelle Graham of CBS News Detroit.
What does a Sun burned retina look like?
As you can see (left) , the top panel is a view of the patient's retina as observed directly from looking into the front of the eye. The lower panel is a an OCT image that shows the layers of the neural retina in cross section. OCT stands for Optical Coherence Tomography, and it is a way to use back-scattered light to see the layers of the retina. Obviously a very useful imaging system for your eye doctor. The green line on the top panel shows the location of the OCT scan.
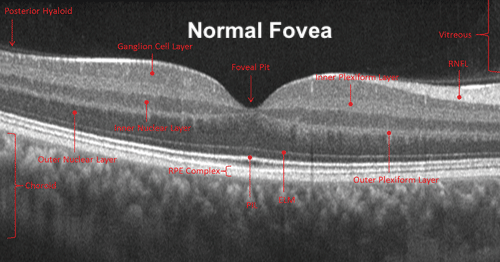
I have added the red arrow, pointing to the OCT image cross-section at the fovea from this patient with a fovea burn. This area is the part of the retina that you are reading this with now, your central, high-detailed, vision. That white stalk of burn damage should not be there. A normal undamaged human fovea does not have that burn feature, as seen in this normal retinal OCT scan below.
So I hope that you were able to watch the Solar Eclipse of April 8th 2024 in a safe manner. My best advice for your vision health at any time is get an eye check-up at least every two years when younger and over 30 years of age it is best to get an eye exam once per year. If you have diabetes or heart disease then you want an eye exam every year regardless of your age. The reality is that most damage to your retina occurs without any sensation or pain, so many conditions affecting your retinas will be detected by your eye exam and catching retinal conditions early is important for possible treatment. Once photoreceptor cells have died, there is nothing currently that modern medicine can do to fix that.
Ken Mitton